Haemoptysis as a presentation of an infected aortic aneurysm rupture
Keywords:
Haemoptysis, Infected aneurysm , Aortobronchial fistula, thoracic endovascular aortic repair (TEVAR)Abstract
Introduction: Infective thoracic aortic aneurysms are uncommon, especially presenting with haemoptysis.
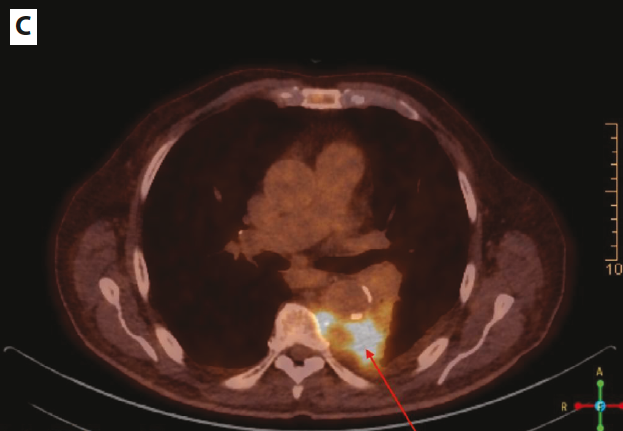
Case presentation: We report the case of an 81-year-old male who presented with fever and pleuritic chest pain and was initially misdiagnosed with community-acquired pneumonia. A CT scan later revealed a saccular, ruptured thoracic aortic aneurysm. Despite antibiotic therapy, the patient developed haemoptysis, necessitating thoracic endovascular aortic repair (TEVAR). Post-procedure, the patient showed significant clinical improvement and was discharged in stable condition 45 days later.
Conclusions: Infected thoracic aortic aneurysms presenting as haemoptysis are exceptionally rare but life-threatening. Early clinical suspicion (manifested by haemoptysis, fever and thoracic pain) is essential, particularly in patients with risk factors such as immunosuppression or previous infections. This case emphasizes the importance of prompt diagnosis and intervention, along with the use of appropriate imaging techniques to reduce morbidity and mortality associated with this rare yet severe condition.
References
1. Osler W. The gulstonian lectures on malignant endocarditis. Br Med J 1885;1:467.
2. Isselbacher EM, Preventza O, Hamilton Black J3rd, Augoustides JG, Beck AW, Bolen MA, et al. Guideline for the diagnosis and management of aortic disease: a report of the american heart association/american college of cardiology joint committee on clinical practice guidelines. Circulation 2022;146:334-482.
3. Sörelius K, Mani K, Björck M, Sedivy P, Wahlgren CM, Taylor P, et al. Endovascular treatment of mycotic aortic aneurysms. A european multicenter study. Circulation 2014;130:2136-42.
4. Cinà CS, Arena GO, Fiture AO, Clase CM, Doobay B. Ruptured mycotic thoracoabdominal aortic aneurysms: a report of three cases and a systematic review. J Vasc Surg 2001;33:861-7.
5. Inoue H, Iguro Y, Yamamoto H, Ueno M, Higashi A, Tao K, et al. Palliative stent-graft insertion followed by an allograft replacement for an infected and ruptured aortic aneurysm. Ann Thorac Cardiovasc Surg 2009;15:261-4.
6. Daitoku K, Fukuda I, Taniguchi S, Minakawa, M. Endovascular treatment of an aortobronchial fistula caused by a distal aortic arch mycotic aneurysm: report of a case. Surg Today 2010;40:54-6.
7. Beiko T, Huggins J. A mycotic aneurysm and a pulmonary nodule in immunocompromised patient: where is occam's razor when you need it?. Chest 2013;144 (meeting abstract): no pagination.
8. Tamura K, Yoshitaka H, Totsugawa T, Tsushima Y, Chikazawa G, Ohno T, et al. Bridge use of endovascular repair and delayed open operation for infected aneurysm of aortic arch. Ann Thorac Surg 2013;96:1471-3.
9. Heneghan RE, Singh N, Starnes BW. Successful emergent endovascular repair of a ruptured mycotic thoracic aortic aneurysm. Ann Vasc Surg 2015;29:843.e1-e.6.
10. Hui DS, Stoeckel DA, Kaufman EE, Jacobs DL. Massive hemoptysis from an aortobronchial fistula secondary to BCG-related mycotic thoracic aortic aneurysm. Ann Thorac Surg 2016;101:350-2.
11. Isbir S, Hamidov A, Seven IE, Ak K. Massive hemoptysis related to contained rupture of syphilitic aortic aneurysm into the pulmonary parenchyma. J Thorac Cardiovasc Surg 2017;154: 23-5.
12. Fernandez L, Gutierrez L, Yara JD. A case of massive hemoptysis secondary to aortobronchial fistula caused by mycotic aneurysm in thoracic aorta: a challenging multidisciplinary therapeutic approach. Am J Respir Crit Care Med 2017;195:1931.
13. Novelli M, Cataldi A, Pilato A, Quadri R, Savoldi S. Tuberculous mycotic aneurysm of the aorta: a case report of haemoptysis. Recenti Prog Med 2018;109:398-400.
14. Wu SJ, Huddin JC, Wanger A, Estrera AL, Buja LM. A case of Brucella aortitis associated with development of thoracic aortic aneurysm and aortobronchial fistula. Cardiovasc Pathol 2019;39:5-7.
15. Liu C-H, Huang S-C, Hsu C-T. A fatal masquerade in pneumonia: ruptured thoracic aortic aneurysm. Clin Case Rep 2022;10:e05285.
16. Tournaye E, Hollering P, De Roover D, Dossche K, Vercauteren SRW. Staphylococcus aureus sepsis and hemoptysis as messengers of a rather impractically located mycotic aneurysm. Acta Chirurgica Belgica 2023;123:430-5.
17. Oderich GS, Panneton JM, Bower TC, Cherry KJ, Rowland CM, Noel AA et al. Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg 2001;34:900-8.
18. Taylor LM, Deitz DM, McConnell DB, Porter JM. Treatment of infected abdominal aortic aneurysms with extra-anatomic bypass, aneurysm excision, and drainage. Am J Surg 1988;155:655-8.
19. Kilic A, Shah AS, Black JH, Whitman GJ, Yuh DD, Cameron DE et al. Trends in repair of intact and ruptured descending thoracic aortic aneurysms in the United States: a population-based analysis. J Thorac Cardiovasc Surg 2014;147:1855-60.
20. Negishi K, Ono Y, Kurosawa K, Takamatsu H, Nakano A, Hasegawa A et al. Infective endocarditis complicated by mycotic aneurysm of a coronary artery with a perforated mitral valvular aneurysm. J Am Soc Echocardiogr 2009;22:542-4.
21. Jarrett F, Darling RC, Mundth ED, Austen WG. Experience with infected aneurysms of the abdominal aorta. Arch Surg 1975;110:1281-6
Published
Issue
Section
License
Copyright (c) 2025 The Author(s)

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Mattioli 1885 has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
How to Cite




